Atrioventricular Septal Defect (AVSD)
 Atrioventricular septal defects are also referred to as AV canal defects and endocardial cushion defects.
Atrioventricular septal defects are also referred to as AV canal defects and endocardial cushion defects.
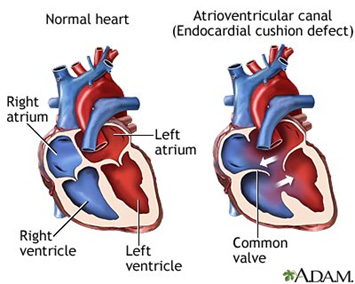
They represent a spectrum of anomalies characterized by varying degrees of incomplete development of the septal tissue surrounding the AV valves in addition to abnormalities of the valves themselves.
Partialor incomplete AVSDs have a crescent-shaped primum ASD, positioned just above the AV valve. Complete AVSDs have both defects in the atrial septum just above the AV valves and defects in the ventricular septum just below the AV valves.
There is a single AV valve bridging the left and right sides of the heart. Intermediateor transitional AVSDs have both an ASD just above and a VSD just below the AV valves but have two distinct left and right AV valve orifices. As many as 50-75% of patients with complete AVSD have Down syndrome, and AVSD is the most common congenital heart defect in Down syndrome. They are also present in almost all patients without a spleen (asplenia).
Presentation depends on the amount of left-to-right shunting and therefore on the pulmonary vascular resistance. Patients with partial AVSDs, and no AV valve regurgitation, may be asymptomatic for years. Patients with complete AVSDs have more left-to-right shunting because of the large VSD. As PVR decreases in the first few weeks of life, patients present with worsening symptoms, especially if there is AV valve regurgitation.
There may be a systolic ejection murmur due to increased flow across the pulmonary valve, a holosystolic apical murmur from left AV valve regurgitation, and murmurs from the ASD and VSD. CXR reveals an enlarged PA and RVH. EKG shows RVH and sometimes LVH. Echocardiography is the diagnostic test of choice. Cardiac cath may be used to measure PVR and determine operability (see below).
Similar to secundum ASD, patients with asymptomatic partial AVSD should be repaired electively by about 5 years of age, and sooner if significant left AV valve regurgitation is present. Repair is typically by closure of the left AV valve cleft and patch closure of the primum ASD. Infants with complete AVSD should undergo repair at 4-6 months of age, and sooner if symptomatic. Contraindications include PVR > 10 units/m2 or PVR:SVR ratio > 0.7. Repair of the complete AVSD must be taken with care to avoid damaging the AV node.