Transposition of the Great Arteries (TGA)
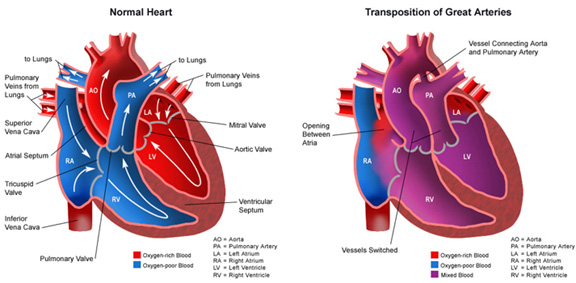
This is the most common of the cyanotic heart diseases. In transposition of the great arteries, the aorta arises from the right ventricle (RV) and the pulmonary artery arises from the left ventricle (LV). Survival is dependent upon mixing, usually by an atrial level connection or ASD. Up to 50% of patients will also have a VSD. The aorta is usually anterior and to the right of the PA. There are a number of configurations of the coronary arteries, which must be considered carefully when planning repair.
Presentation depends on the presence of associated cardiac anomalies. If there is no VSD, cyanosis will be more pronounced and may be present at birth. On the other hand, if there is a significant VSD, cyanosis will develop later and heart failure may be the predominant clinical finding. Most patients with TGA and intact ventricular septum have a soft systolic murmur. The EKG will show increasing RVH or biventricular hypertrophy over time. CXR shows an egg-shaped heart, narrow superior mediastinum, and increased pulmonary vascular markings with cardiomegaly. Echocardiography confirms the diagnosis and defines associated atrial and ventricular defects, valve function, pulmonary stenosis, and coronary configuration. Cardiac catheterization is usually reserved for those patients requiring balloon septostomy (patients born without mixing defects like an ASD or VSD- see below).
TGA is the most common congenital heart defect requiring early intervention. Currently, anatomic correction is performed early in life using the arterial switch operation. Since the LV is ejecting against the lower resistance pulmonary circulation, the repair must be carried out early or the LV will fail to thicken and be unable to support the systemic circulation following the switch. If LV pressure has already fallen to less than 60% of systemic, a two-staged approach involving initial PA banding may be used. The PA band restricts pulmonary blood flow and causes the LV to work harder, allowing for growth and thickening. For infants with hemodynamic instability or persistent hypoxemia or acidemia shortly after birth, balloon atrial septostomy, performed percutaneously in the cardiac catheterization lab, may be employed to improve mixing. The arterial switch operation involves division of the PDA, transection of the great vessels, transfer of the coronary arteries as buttons of tissue to the new aorta, and closure of any defects.