Brain Aneurysm Treatment
Brain aneurysms, also known as cerebral aneurysms or intracranial aneurysms, are areas of weakness in a brain blood vessel. Over time, the pressure in a vessel can cause the weak area to grow larger and thinner, like a bulge in a water hose, until the vessel ruptures. Brain aneurysms usually occur in the large blood vessels located at the base of the brain, where the blood flow is highest. When aneurysms bleed, the blood accumulates in the fluid space under the brain known as the subarachnoid space and the bleeding is called a subarachnoid hemorrhage. Aneurysms that bleed are life-threatening and should be treated urgently.
Approximately 10–12 million people in the USA have brain aneurysms and about 27,000 new aneurysms are discovered each year [1]. Aneurysms are most commonly diagnosed in patients between the ages of 30 and 60.
Types of Aneurysms
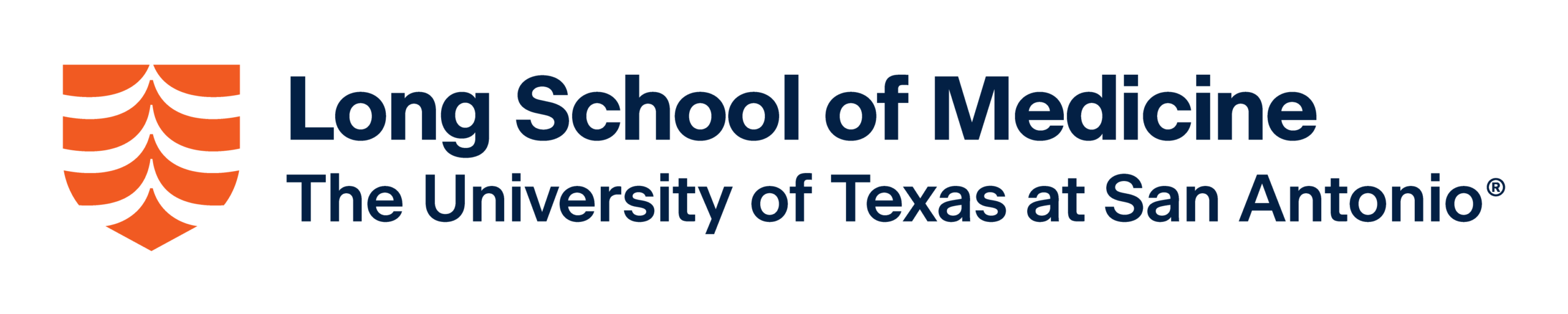
There are two main types of aneurysms that lead to subarachnoid hemorrhage: saccular aneurysms and fusiform aneurysms.
- Saccular Aneurysms (or Berry Aneurysms) are the most common type of aneurysm, accounting for 80–90% of all brain aneurysms. These aneurysms are bulges on the wall of a blood vessel that have the appearance of a blister, sac, or berry (FIG1a). They can often be treated using surgical or endovascular techniques.
- Fusiform Aneurysms are rare, sausage-like expansions of the entire blood vessel on all sides (FIG1b). These aneurysms can be difficult to treat, but they rarely rupture
Although they are uncommon, two additional types of aneurysm exist. Mycotic aneurysms can arise from bacterial infections in brain blood vessels. They are usually treated with antibiotics but may require surgical intervention if they have ruptured. Dissecting aneurysms (or blister aneurysms) can result from a tear in the inside wall of the blood vessel. Their risk of rupture is high, so they need to be treated quickly.
Credit: openi.nlm.nih.gov
Risk of Rupture
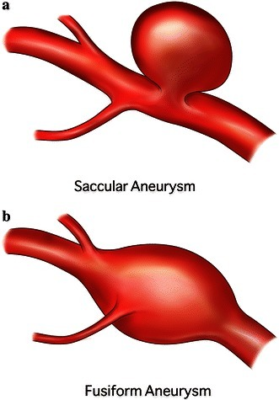
Size and location are generally the most important factors that determine the likelihood that an aneurysm will rupture. Small aneurysms (less than five millimeters in size) are unlikely to rupture. They are often not treated at all unless they begin to grow. The larger an aneurysm is, the higher the chance it will bleed (Table 1) and the more likely it will need treatment.
The location of an aneurysm is also important. Aneurysms on blood vessels located in the back half of the brain (vertebral arteries, the basilar artery, and the posterior communicating artery) are at higher risk of bleeding than aneurysms found on blood vessels in the front half of the brain (the carotid artery, the middle cerebral artery, and the anterior cerebral artery). Other factors that are thought to increase the likelihood of a rupture include: the presence of multiple aneurysms (RINKEL META-Analysis), aneurysm growth, symptoms of aneurysm leak or nerve compression, having a previous aneurysm rupture, irregular aneurysm wall outpouchings, and a strong family history of aneurysm rupture.
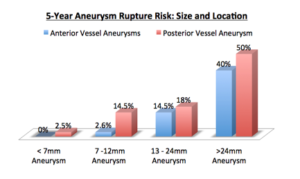
TABLE 1. The rupture rate for aneurysms of different size ranges based on location of blood vessels at the front part of the brain (anterior circulation) or the back part of the brain (posterior circulation) [2]. Risk of rupture is higher for larger aneurysms; aneurysms in the back of the brain are at higher risk than those in the front.
Diagnosis
Aneurysms are typically identified through the use of medical imaging techniques. The most common tests used to evaluate a brain for aneurysms include:
- Magnetic Resonance Imaging Angiogram (MRA) – Uses shifting magnetic fields to create images of the brain and the brain’s blood vessels. High quality images of the brain and moderate quality images of the blood vessels can be obtained with MRA.
- Computed Tomography Angiogram (CTA scan) – uses multiple X-ray images taken from different angles to produce cross-sectional pictures of the brain and brain blood vessels. To see blood vessels more accurately with CT scans, contrast dye must be injected into the patient’s veins through an IV, usually in the arm. Moderate quality images of the brain and good quality images of the blood vessels can be obtained with CTA (Figure 2 a, b).
- Cerebral Angiogram (Digital Subtraction Angiography) – Small tubes are placed inside the arteries of the leg where they are advanced into the arteries of the neck using X-ray guidance. Dye is then injected through the tubes. It flows with the blood through the neck arteries into the brain blood vessels. Highest possible quality images of the neck and brain blood vessels can be captured using this technique (Figure 2 c, d).
Multiple views of the same ruptured left middle cerebral artery aneurysm using two different imaging techniques: CTA (a,b) and cerebral angiogram (c,d). Note the higher clarity of the vessels on the cerebral angiogram compared to the CTA.
Treatment Options
There are 2 primary techniques to treat brain aneurysms:
1. Surgical Clipping
Surgical treatment for aneurysms involves opening the skin and bone over the surface of the brain. This allows the surgeon to carefully dissect under the brain (or between the lobes of the brain depending on the location of the aneurysm) and place a metal clip across the “neck” or base of the aneurysm (Figure 3). The clip blocks blood from entering but keeps the normal artery open. Once an aneurysm is clipped, it will become isolated from normal blood circulation and shrink in size until it is undetectable, a process known as aneurysm obliteration. Once aneurysm obliteration is confirmed via imaging, patients are considered permanently cured. During these surgeries, the patient’s brain is touched with minimal frequency.
 FIGURE 3a. A small aneurysm clip next to a penny for scale.
FIGURE 3a. A small aneurysm clip next to a penny for scale.
FIGURE 3b. The outline of a typical craniotomy for aneurysm clipping
2. Endovascular Treatment (Interventional Treatment) Certain aneurysms with favorable locations and shapes can be treated from inside the blood vessel via small catheters and tubes. Using X-ray guidance, small tubes can be navigated into the brain blood vessels to occlude aneurysms. The three most common ways to treat an aneurysm from inside the vessel are: Endovascular Coiling – Small metal coils are pushed through the tubes and delivered into the aneurysm, thereby blocking blood from entering and preventing future rupture (Figure 4) Endovascular Stent-assisted Coiling – A small metal stent is placed in the vessel across the base of the aneurysm to protect it from the coils that are delivered into the aneurysm through the tubes. Endovascular Flow Diversion – A metal stent with narrow holes is placed across the base of an aneurysm. The stent diverts blood flow away from the aneurysm and encourages it to stay in the vessel. Over several months, the blood in the aneurysm clots due to slow flow and the aneurysm heals, but the normal vessel stays open. This technique is often used for very large aneurysms or aneurysms that are difficult to treat with coiling or surgery.
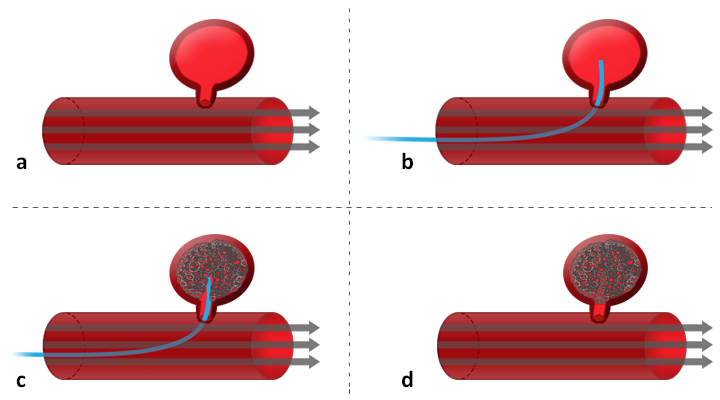 FIGURE 4. A diagram of the steps of endovascular aneurysm coiling showing: a) an aneurysm prior to treatment b) a catheter placed inside the aneurysm c) coils being pushed through the catheter to fill the aneurysm d) the final state after aneurysm after coiling with the aneurysm now filled with metal coils and the main vessel open. Brain blood vessel specialists are the physicians who can best determine whether or not a brain aneurysm requires treatment and, if it does, which approach is best to implement. Such specialists include: cerebrovascular neurosurgeons, neurologists or neurointerventional radiologists. Factors that help physicians determine the best treatment option for an individual patient include: Ruptured vs. unruptured aneurysm Patient age, overall health, and medical history Symptoms Risk of aneurysm rupture Size, location and type of the aneurysm Individual tolerance for procedures Patient preferences Physician expertise and experience Depending on the exact nature of an aneurysm, the individual factors listed above, and the patient’s input, cerebrovascular specialists will make the recommendation that they feel is best tailored to each patient’s individual circumstance.
FIGURE 4. A diagram of the steps of endovascular aneurysm coiling showing: a) an aneurysm prior to treatment b) a catheter placed inside the aneurysm c) coils being pushed through the catheter to fill the aneurysm d) the final state after aneurysm after coiling with the aneurysm now filled with metal coils and the main vessel open. Brain blood vessel specialists are the physicians who can best determine whether or not a brain aneurysm requires treatment and, if it does, which approach is best to implement. Such specialists include: cerebrovascular neurosurgeons, neurologists or neurointerventional radiologists. Factors that help physicians determine the best treatment option for an individual patient include: Ruptured vs. unruptured aneurysm Patient age, overall health, and medical history Symptoms Risk of aneurysm rupture Size, location and type of the aneurysm Individual tolerance for procedures Patient preferences Physician expertise and experience Depending on the exact nature of an aneurysm, the individual factors listed above, and the patient’s input, cerebrovascular specialists will make the recommendation that they feel is best tailored to each patient’s individual circumstance.Future Direction in Therapy
Engineers and physicians are continuously working on new technologies to better diagnose and treat brain aneurysms. Endovascular therapies, in particular, are rapidly evolving. Each year more aneurysms can be safely and effectively treated from inside the blood vessel, Surgeons at the UT Health Science Center for Cerebrovascular and Endovascular Surgery have achieved the highest level of surgical and endovascular training, which allows them to approach brain aneurysms from either inside or outside the vessel, depending on the best treatment strategy for the patient. Scientists inside and outside UT are working hard to better understand the causes behind aneurysm formation with the ultimate goal of developing non-surgical treatments for brain aneurysms that will be less invasive for patients.
References
- Brisman, JL; Song, JK; Newell, DW (Aug 31, 2006). “Cerebral aneurysms.”. The New England Journal of Medicine 355 (9): 928–39. doi:10.1056/nejmra052760. PMID 16943405
- The International Study of Unruptured Intracranial Aneurysms Investigators: Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362:103-110, 2003