Parkinson’s Disease
(also known as PD) is a degenerative disorder of the central nervous system that often impairs the sufferer’s motor skills and speech.
Parkinson’s disease belongs to a group of conditions called movement disorders. It is characterized by muscle rigidity, tremor, a slowing of physical movement ( bradykinesia) and, in extreme cases, a loss of physical movement ( akinesia). The primary symptoms are the results of decreased stimulation of the motor cortex by the basal ganglia, normally caused by the insufficient formation and action of dopamine, which is produced in the dopaminergic neurons of the brain. Secondary symptoms may include high level cognitive dysfunction and subtle language problems. PD is both chronic and progressive.
While many forms of parkinsonism are “idiopathic” (cause unknown), “secondary” cases may result from drug toxicity, head trauma, or other medical disorders.
Signs and Symptoms
Parkinson disease affects movement (motor symptoms). Typical other symptoms include disorders of mood, behavior, thinking, and sensation (non-motor symptoms). Individual patients’ symptoms may be quite dissimilar and progression of the disease is also distinctly individual. The cardinal symptoms are:
- Tremor: Normally 4-7 Hz tremor, maximal when the limb is at rest, and decreased with voluntary movement. It is typically unilateral at onset. This is the most apparent and well-known symptom, though an estimated 30% of patients have little perceptible tremor.
- Rigidity: stiffness; increased muscle tone. In combination with a resting tremor, this produces a ratchety, “cogwheel” rigidity when the limb is passively moved.
- Bradykinesia / Akinesia: respectively, slowness or absence of movement.
- Postural instability: failure of postural reflexes, which leads to impaired balance and falls.
- Gait disturbances: Shuffling, decreased arm-swing, gait freezing.
Diagnosis
There are currently no blood or laboratory tests that have been proven to help in diagnosing PD. Therefore the diagnosis is based on medical history and a neurological examination. The disease can be difficult to diagnose accurately. The Unified Parkinson’s Disease Rating Scale is the primary clinical tool used to assist in diagnosis and determine severity of PD. Early signs and symptoms of PD may sometimes be dismissed as the effects of normal aging. The physician may need to observe the person for some time until it is apparent that the symptoms are consistently present. Usually doctors look for shuffling of feet and lack of swing in the arms. Doctors may sometimes request brain scans or laboratory tests in order to rule out other diseases. However, CT and MRI brain scans of people with PD usually appear normal.
Pathology
The symptoms of Parkinson’s disease result from the loss of pigmented dopamine-secreting (dopaminergic) cells in the pars compacta region of the substantia nigra (literally “black substance”). These neurons project to the striatum and their loss leads to alterations in the activity of the neural circuits within the basal ganglia that regulate movement. The lack of dopamine results in increased inhibition of the ventral lateral nucleus of the thalamus, which sends excitatory projections to the motor cortex, thus leading to hypokinesia.
Treatment
Parkinson’s disease is a chronic disorder that requires broad-based management including patient and family education, support group services, general wellness maintenance, physiotherapy, exercise, and nutrition. At present, there is no cure for PD, but medications or surgery can provide relief from the symptoms.
Levodopa
The most widely used form of treatment is L-dopa in various forms. L-dopa is transformed into dopamine in the dopaminergic neurons. However, only 1-5% of L-DOPA enters the dopaminergic neurons. The remaining L-DOPA is often metabolized to dopamine elsewhere, causing a wide variety of side effects. Carbidopa and benserazide are dopa decarboxylase inhibitors. They help to prevent the metabolism of L-dopa before it reaches the dopaminergic neurons and are generally given as combination preparations of carbidopa/levodopa (e.g. Sinemet, Parcopa) and benserazide/levodopa (e.g. Madopar).
There are also controlled release versions of Sinemet and Madopar that spread out the effect of the L-dopa. Duodopa is a combination of levodopa and carbidopa, dispersed as a viscous gel. Using a patient-operated portable pump, the drug is continuously delivered via a tube directly into the upper small intestine, where it is rapidly absorbed. There is also Stalevo (Carbidopa, Levodopa and Entacapone). Entacapone inhibits the COMT enzyme, thereby prolonging the effects of L-dopa, and so has been used to complement L-dopa. Mucuna pruriens, is a natural source of therapeutic quantities of L-dopa, and has been under some investigation.
Dopamine Agonists
The dopamine-agonists bromocriptine, pergolide, pramipexole, ropinirole , cabergoline, apomorphine, and lisuride, are moderately effective. Dopamine agonists initially act by stimulating some of the dopamine receptors. Dopamine agonists can be useful for patients experiencing on-off fluctuations and dyskinesias as a result of high doses of L-dopa. Apomorphine can be administered via subcutaneous injection using a small pump carried by the patient. A low dose is automatically administered throughout the day, reducing the fluctuations of motor symptoms by providing a steady dose of dopaminergic stimulation.
MAO-B Inhibitors
Selegiline and rasagiline reduce the symptoms by inhibiting monoamine oxidase-B (MAO-B), which inhibits the breakdown of dopamine secreted by the dopaminergic neurons.
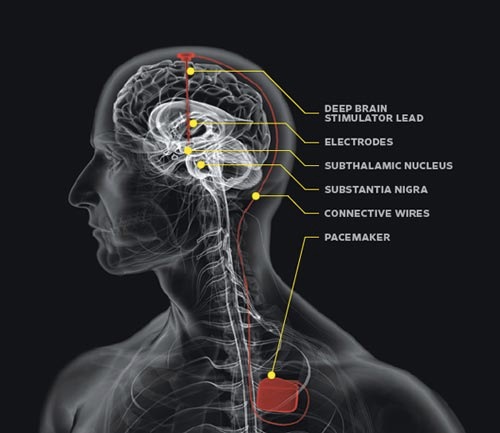
Surgery and Deep Brain Stimulation
Treating Parkinson’s disease with surgery was once a common practice, but after the discovery of levodopa, surgery was restricted to only a few cases. Studies in the past few decades have led to great improvements in surgical techniques, and surgery is again being used in people with advanced PD for whom drug therapy is no longer sufficient.
Deep brain stimulation is presently the most used surgical means of treatment.