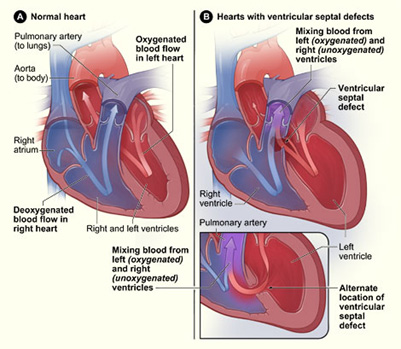
Ventricular Septal Defect
VSD is the most common congenital heart defect, comprising 20-25% of all lesions and occurring in association with other defects about 50% of the time. Classification is based upon the location of the defect in the interventricular septum. The most common type is the membranous defect, located in the membranous septum directly under the aortic valve, near the bundle of His. Muscular defects are located in the muscular and apical portion of the ventricle and are the most common type of uncomplicated VSD (isolated VSD without associated lesions). Multiple muscular defects may be present, constituting a “Swiss-cheese” type of VSD. Infundibular defects (also referred to as conal, subpulmonary, subarterial, and supracristal) are located just below the pulmonic valve. This type may cause aortic insufficiency.
Patients with small defects may be asymptomatic and diagnosed only secondary to a loud murmur at the left lower sternal border (smaller VSD = usually louder murmur). The murmur is usually not audible just after birth as the pulmonary vascular resistance (PVR) is too high to allow for a significant left-to-right shunt. Patients with larger defects may present with heart failure. CXR will show increased pulmonary vascularity and possible cardiomegaly. Echocardiography is used to define the defect(s) and cardiac catheterization is not routinely performed but can be used for device closure or to investigate pulmonary vascular resistance or response to vasodilators.
The majority of small membranous and muscular VSDs will close spontaneously, and as such, asymptomatic patients may just be followed. However, infants with heart failure symptoms despite medical / pharmacologic therapy require VSD closure. Children older than one year of age with pulmonary artery pressures greater than one half that of systemic pressure require repair. All VSDs associated with aortic regurgitation should be repaired. In adults, VSDs should be repaired when symptoms are present or the Qp:Qs ratio is > 1.5:1. Fixed pulmonary vascular hypertension precludes operative repair.